 New Business Inquiries (877) 305-7933
New Business Inquiries (877) 305-7933- Manage Account. external page
- Other Languages
Biosimilars can significantly reduce employer pharmacy costs. Are you missing out?


With pharmacy costs accounting for almost 25% of total health care expenses, it’s no surprise drug prices are top of mind for employers.1 Specialty drugs are a major contributor, with businesses paying an extra $38,000 per year for each employee who needs them.2
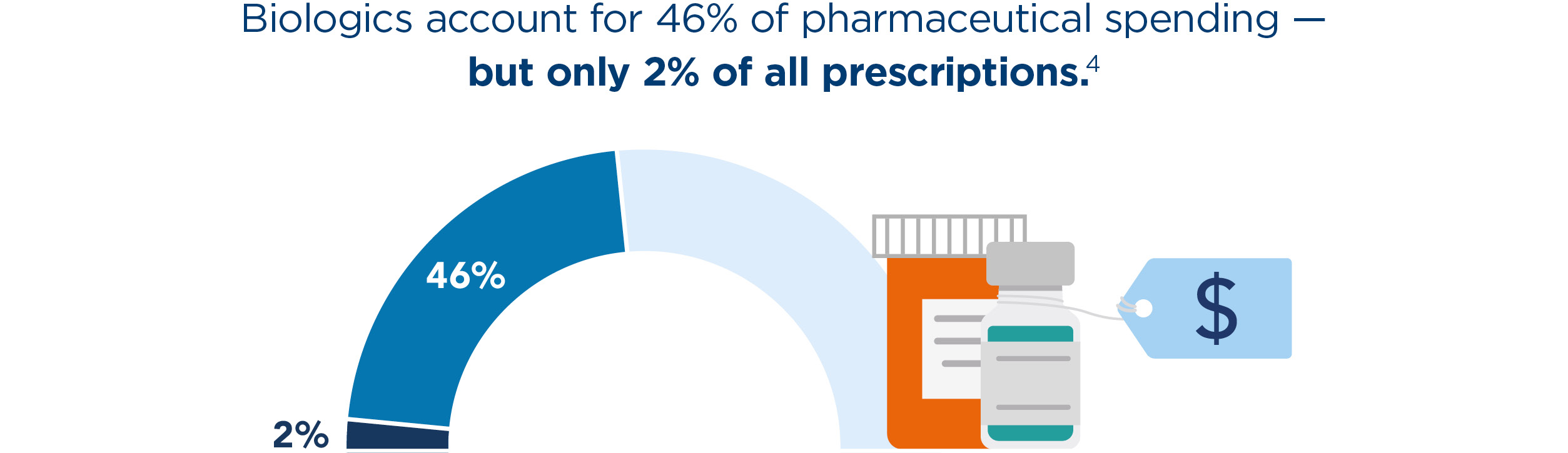
Biologics are a class of specialty drugs that treat chronic conditions like cancer, diabetes, rheumatoid arthritis, multiple sclerosis, and Crohn’s disease. They’re also incredibly expensive. To put that into perspective, the U.S. spent $568 billion on pharmaceuticals in 2021 — and $260 billion went toward biologics.3 And while biologics make up nearly half of the nation’s annual drug spend, they represent a mere 2% of all prescriptions. However, there are safe, effective, and more affordable alternatives to biologics: Biosimilars.

Biosimilars are the future of specialty drug therapy
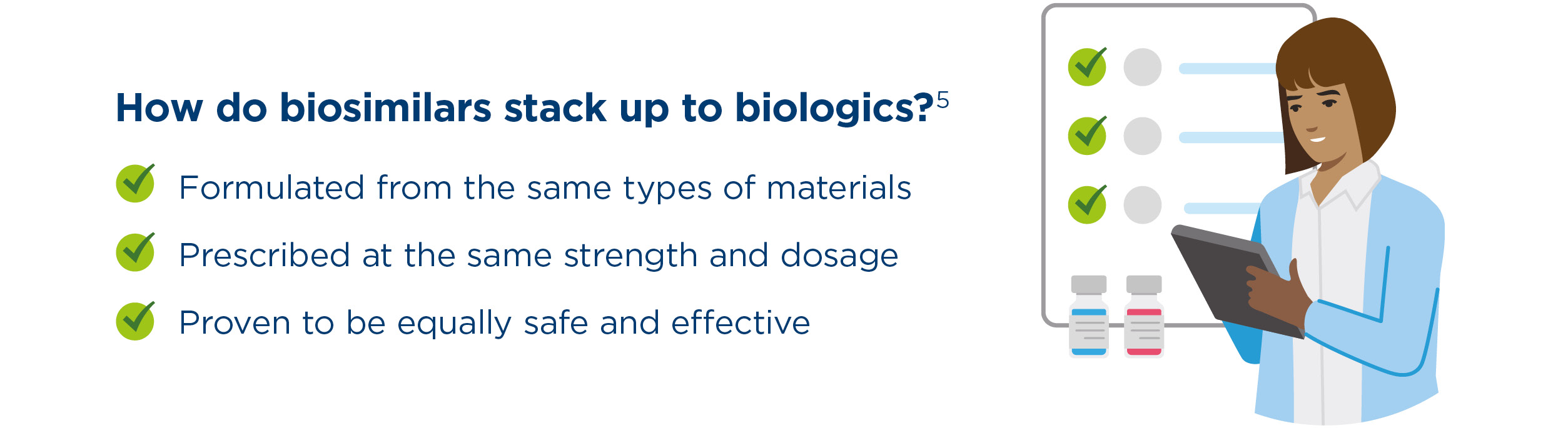
Biosimilar medications are safe, effective, and closely mimic the biologics they’re based on. The Food and Drug Administration (FDA) ensures that all biosimilars undergo rigorous reviews and approvals before going to market. “Biosimilars are not identical to biologics, so there’s a perception that they won’t work as well,” explains David M. Chen, Kaiser Permanente’s director of Drug Use Management. “But clinical studies and real-world trials have proven that biosimilars are just as safe and effective as brand biologics.”

Biosimilars are more affordable — and driving down biologic costs
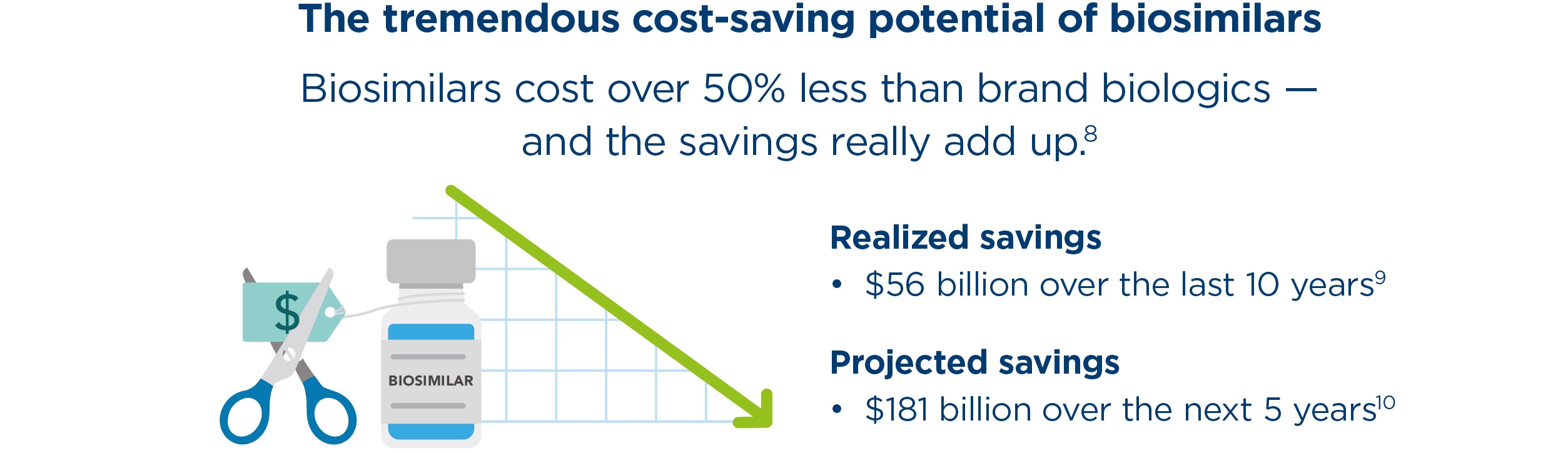
On average, biosimilars cost 50% less than their biologic reference products.6 Biosimilars are also driving down biologic costs by creating competition — with the average price of brand biologics falling 25% after biosimilar launch.7 “If biosimilars were more widely adopted, the cost of health care wouldn’t rise so rapidly,” Chen says.

Biosimilars for cancer — a prime example of the savings at stake
Cancer is a leading driver of employer health care costs. Since the advent of oncology biosimilars, oncology spending growth has slowed by 50%.11 Imagine the impact if more doctors were prescribing them?

Why are biosimilars dramatically underutilized?
Adoption is disincentivized
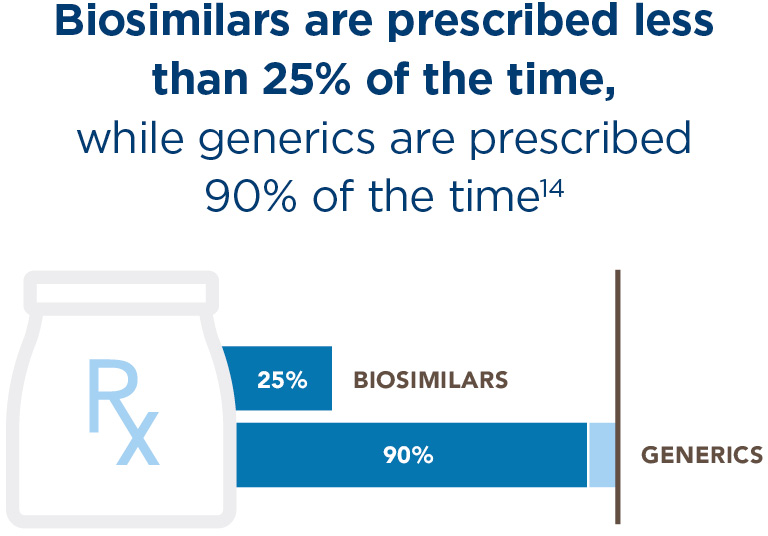
Biosimilar adoption is higher in settings where prescribers are incentivized for improving quality while lowering costs, such as value-based care organizations. Unfortunately, prescribers outside these systems have been slow to adopt biosimilars and many health plans make biosimilars difficult to access because they’re financially disincentivized. A 2023 study showed that biosimilars are covered more restrictively than biologics about 20% of the time — and plans are more likely to restrict coverage on biosimilars that treat the most common conditions.12
Pharmacy benefit managers (PBMs) often use their bargaining power to negotiate discounts or rebates from biologics manufacturers, thereby disincentivizing adoption of biosimilars. It’s a complicated financial system driving profits for drug companies — with businesses, consumers, and health care organizations ultimately paying the price.
Prescribers need accurate information
Currently, it can be difficult to access unbiased information about biosimilars. Former FDA Commissioner Scott Gottlieb expressed concerns about, “either deliberate or unintentional efforts by branded companies to create confusion” around the safety of biosimilar drugs.13 But when prescribers understand the facts about biosimilars — and are not incentivized to stick with biologics — adoption increases exponentially.
Humira biosimilar could save billions, but adoption remains low*
Amjevita is a new biosimilar for the notoriously expensive biologic Humira — the best-selling drug in history — used to treat common chronic conditions like rheumatoid arthritis and psoriasis.* Given that employers spent $15 billion on Humira in 2020 alone, this is one of the most exciting biosimilar launches to date.15 Despite significant cost savings — Kaiser Permanente projects $300 million in savings by simply transitioning 90% of their patients to Amjevita — adoption of Amjevita is currently about 9%.16
How employers can reap the cost-saving benefits of biosimilars now
Employers who want to fully optimize cost savings from biosimilars must actively engage in the benefits design process. “Employees with chronic conditions need access to more affordable medications — like biosimilars. Employers can absolutely help make that happen,” Chen says.

It’s essential for employers to make sure biosimilars are:
- Included in plan design as preferred products on a generic-like tier
- Listed on the formulary as covered products
- Affordable to employees with low or no copays
3 ways employers can help drive biosimilar adoption forward
One solution is to choose a health plan with a history of embracing and encouraging biosimilar adoption, who can demonstrate how that approach saves their customers money. There are also things you can do to influence your current health plan in a positive direction.
- Understand your health plan’s biosimilar strategy. Are they set up to make biosimilar adoption easy and seamless, or are they creating barriers?
- Identify potential savings. Ask your health plan to run anonymous reports to see how many employees might be candidates for biosimilars and help evaluate the potential savings.
- Take control of the formulary. Request the adoption of a biosimilar preferred formulary — or create a custom/carved-out formulary that is not rebate-driven.
The future of biosimilars
As more biosimilars reach the market, they’ll increase competition and continue to drive down prices — making essential drug therapies more accessible and affordable.
Insulin biosimilars will revolutionize diabetes management
Minimizing common and costly complications related to diabetes depends on employees taking their medications as prescribed. However, costs are a major hurdle. Right now, 55% of insulin users spend more than $50 per month on insulin — and some pay $400 per month or more.17 As a result, nearly 1 in 5 say they either skip doses, take less than prescribed, or delay refilling prescriptions due to cost.18 Insulin biosimilars promise to help ease this burden — with several already on the market and 9 more currently in development.
“Diabetes is so prevalent, and the cost of insulin has always been a barrier to people managing their symptoms,” says Chen. “If we have more accessibility because insulin biosimilars are more affordable, adherence will go up, and employees will get healthier.”
New interchangeables will remove red tape and automate biosimilar adoption
When a biosimilar is interchangeable, it means pharmacists can swap a more affordable biosimilar for a biologic without consulting the prescriber. Sound familiar? It’s the same as a pharmacist substituting a generic medicine for a branded drug when filling a prescription. However, only a handful of biosimilars are currently approved as interchangeable in the U.S. So it will take time for policy to catch up with science. As more biosimilars become interchangeable, employees with chronic conditions will have one less barrier to more affordable drugs that can keep them healthier and more productive at work.
Employers play a key role in unlocking the full potential of biosimilars
Biosimilars offer much-needed alternatives to the expensive biologics that have made accessing essential drug therapies difficult for employees and expensive for businesses. But employers can help reverse the trend of underutilization and get these life-changing drugs into more employees’ hands — improving workforce health, productivity, and engagement while driving overall health care costs down.
About our expert

David Chen, Pharm D is the director for Drug Utilization Management and the national lead of Clinic Administered Medications and Specialty Products. In this role, he has strategic oversight over cost-effective prescribing and optimal use of preferred therapies. Previously, he has held roles in pharmacy clinical operations, drug education, and ambulatory care all within Kaiser Permanente.
David holds a doctorate in pharmacy from the University of California, San Francisco and completed a PGY1 residency at the Veteran Affairs, San Francisco.
You might also like



*Kaiser Permanente does not endorse the medications or products mentioned. Any trade names listed are for easy identification only.
- 1
“Large Employer Health Care Strategy Survey,” Business Group on Health, 2023.
- 2
Paul Fortunato, “Specialty Drugs: Employers Are Weary (And For Good Reason),” ALM Benefits Pro, June 29, 2023.
- 3
“Biosimilars in the United States 2023–2027,” The IQVIA Institute for Human Data Science, January 31, 2023.
- 4
See note 3; Jessica Chang et al., “Uptake of Biosimilars Remains Low Among People with Employer-Sponsored Insurance,” Health Care Cost Institute, March 30, 2023.
- 5
“Biosimilar Basics for Patients,” FDA.gov, August 10, 2023.
- 6
“The U.S. Generic & Biosimilar Medicines Savings Report: September 2022,” Association for Accessible Medicines, September 2022.
- 7
See note 6.
- 8
See note 6.
- 9
See note 3.
- 10
See note 3.
- 11
See note 6.
- 12
Tianzhou Yu et al., “Factors Associated with Biosimilar Exclusions and Step Therapy Restrictions Among US Commercial Health Plans,” BioDrugs, p. 37 (2023).
- 13
Christopher Rowland, “‘Marketers Are Having a Field Day’: Patients Stuck in Corporate Fight Against Generic Drugs,” The Washington Post, January 9, 2019.
- 14
See note 3; “Office of Generic Drugs 2021 Annual Report, FDA.gov, February 14, 2022.
- 15
Leslie Walker et al., “AbbVie’s Blockbuster Drug Humira Finally Loses its 20-year, $200 Billion Monopoly,” NPR, January 31, 2023.
- 16
“Biosimilars at Kaiser Permanente: Lessons in successfully reducing spending on prescription drugs,” Kaiser Permanente Institute for Health Policy, July 16, 2023; Yaashu Malhotra, “The AMJEVITA impact: Innovative U.S. biosimilar pricing models,” Clarivate, July 5, 2023.
- 17
“Biosimilar Insulin Treatment: What the Science Says.” Endocrine.org, September 28, 2022.
- 18
Adam Gaffney et al., “Prevalence and Correlates of Patient Rationing of Insulin in the United States: A National Survey,” Annals of Internal Medicine, November 2022.
- 19
Jared Ortaliza et al., “How Do Health Expenditures Vary Across the Population?” Peterson-KFF Health System Tracker, November 12, 2021.


